Imagine I take a bunch of 69 to 81 year old dudes and I stack them into quartiles based on testosterone concentrations.
What do you think is going to come up? Will those with higher testosterone be more or less “healthy”?
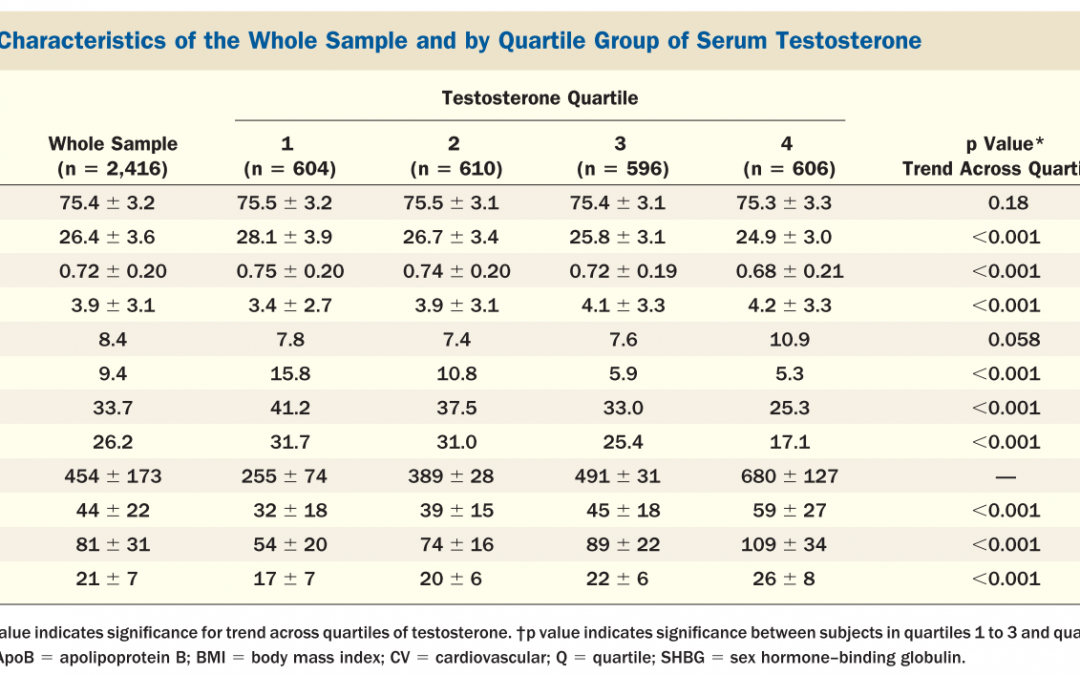
Well that is exactly what Ohlsson et al did with 2,416 men.
And look what they found.

**these were individual t-tests, which should have been a MANOVA or at least had a bonferroni adjustment.
Those in the highest quartile were slightly more active, had better lipids, less diabetes, less hypertension, less history of CVD, higher SHBG (above normal range), and slightly higher estradiol (still well in normal range).
That is kind of a Duh! You just used testosterone to select for a healthier population. This is called healthy user bias and as much as you try to control for it with covariates, you can never account for all of them. For instance, just to name a few that were unaccounted for, there were no variables for mental health, digestion, sleep, thyroid status, F&V consumption, resistance training, happiness, contentment, sexual encounters per week, immune status, and if you give me enough time I could probably think of 50 more.
BUT, this is likely the only longitudinal research of this type that we are going to get and I am not dogging it at all! This data set was likely insanely time consuming to collect.
Now what do you think is going to happen if you add another layer AKA you follow this population over time, say five years…who is going to have more cardiovascular events?
“In this prospective population-based study of elderly Swedish men followed for 5 years, both serum total testosterone and SHBG levels were inversely associated with the risk of cardiovascular events.”
So what do we take away from this study?
It is likely, on average better to maintain a testosterone value above 550 ng/dL throughout your life cycle.
But, can you infer from this data that increased testosterone is cardioprotective?
Absolutely Not!
Can you infer that those who have a testosterone value above 550 ng/dL have better mitochondrial function?
No, but that is a cool hypothesis (of an intervening variable) that could mechanistically connect the dots between these findings.
Can you infer anything about TRT and heart disease from this research?
No – I have discussed this topic at length. It was posted on June 9th, 2017
Every study has positives and negatives and I got my scientific ego bashed in for half a decade to learn how to attempt to break down research and I still have a lot of room to improve. One of my papers for hit with well over 100 revisions from co-authors and editors. For three of those revisions, I basically had to rerun the entire analysis and rewrite the multiple parts of the paper.
Guess how much time RDs, NDs, DOs, MDs, or other some other terminal degree have spent really learning about research? My guess zero hours. Maybe, just maybe they took one four credit course on research design. I might naively and egotistically 100% wrong.
I can’t diagnose or treat anything and I can’t sew your arm back on, but I know how to learn and have been repeatedly advised (email beaten) into questioning everything always.
No matter the credentials, if you are following someone and they are not layering in context and unknowns into their ‘science-y” writing on a regular basis, I would stop following them.
Can’t you just see the headline…
Testosterone = Less Heart Attacks!
And then I or someone like me just might spend time on a Saturday breaking this study down, but searching for black and white “answers” is the real problem. That is why I am writing this to try to motivate people to break out of the myopic cave that our mind always wants to run back to, or at least make one person think twice before they swallow the headlines whole.
Recent Comments